.svg)
Turing Test for Drug Discovery: AI Agents for Translational Readiness
Swapnil Chakraborty

April 29, 2026
The biopharma industry is stuck with promises about Artificial Intelligence. Yet, if we look past the theoretical benchmarks and technology demos, a ground reality remains constant. 90% of drug candidates entering Phase I clinical trials still fail to reach approval. R&D costs continue to rise despite a decade of AI investment, and only 5% of AI pilot programs actually achieve revenue acceleration.
The industry is suffering from a Capability-Value Gap. AI models that score perfectly on curated training datasets frequently collapse when they encounter Out-of-Distribution (OOD) data, such as a completely new patient population or an unseen cell line.
To achieve true translational readiness, we need a new standard of evaluation. This is the idea behind the Turing Test for Drug Discovery (T2D2), a pragmatic framework that shifts the question from "Can AI do this?" to "Where can AI be trusted to improve real discovery decisions?".
To see how T2D2-validated AI agents are actually moving the needle, we have to look at the most critical driver of clinical success today, i.e, biomarker-driven patient stratification.
To understand what AI must achieve, we should look at the gold standard of precision medicine - Merck’s KEYTRUDA® (pembrolizumab). Keytruda is an anti-PD-1 monoclonal antibody that removes the inhibition of the immune response. However, its clinical and commercial efficacy is intrinsically tied to biomarker testing.
Keytruda's potency is not universal and is highly dependent on identifying the right patient subpopulations. For example:
Finding, validating, and establishing clinical cutoff levels for biomarkers like PD-L1 and MSI-H took years of fragmented human effort across genetics, pathology, and clinical trial teams. The true test for modern AI is whether it can replicate and accelerate this exact process to find the next PD-L1, and that is where T2D2 comes in.
Traditional, single-model AI struggles to find complex biomarkers because the data is siloed across biological scales, from spatial transcriptomics and chemoinformatics to clinical trial outcomes.
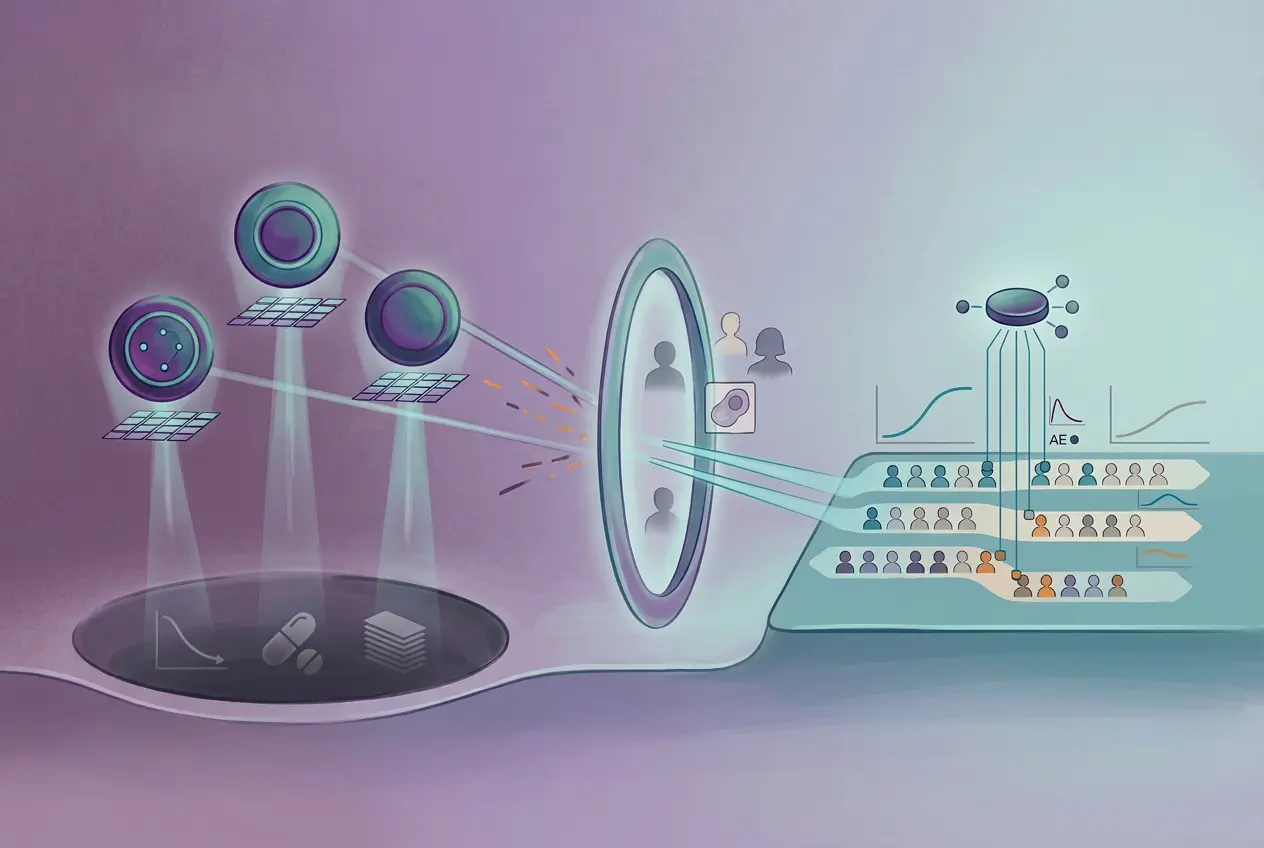
To pass the T2D2, AI must operate like a cross-functional human research organization. This is achieved through Agentic AI, a coordinated team of specialized Large Language Models (LLMs) equipped with domain-specific tools. In a "Virtual Biotech" framework, a model receives a human query and delegates sub-tasks to a team of specialized AI scientists.
This multi-agent architecture allows different models to handle different pieces of the biomarker puzzle:
How does this translate to measurable impact? Consider the real-world example of a Phase II clinical trial (MOONGLOW) testing an OSMRβ-targeted monoclonal antibody (vixarelimab) for ulcerative colitis, which was terminated due to futility.
When a multi-agent AI system analyzed this failure, it didn't just read the top-line results. The Clinical Trial agent noted that the trial enrolled a treatment-refractory cohort but critically lacked OSMR-based stratification, meaning many enrolled patients likely did not have the target pathway active at baseline.
To investigate, the AI agents:
The AI's conclusion? The drug didn't necessarily fail; the trial design did. The agents proposed a revised, biomarker-guided enrollment strategy specifically targeting patients with elevated OSMR, mirroring the exact playbook used by PD-L1 in NSCLC and HER2 in breast cancer.
When AI can successfully perform these complex, multi-step translational tasks, the ROI is staggering. In an autonomous analysis of 55,984 clinical trials, AI agents discovered that drugs targeting highly cell-type-specific genes were:
The era of AI as a simple chatbot or "Automated Research Assistant" is ending. We are moving toward Level 3 maturity of making Autonomous Scientific Partners capable of full agentic discovery.
However, these systems will not replace scientists. Instead, by passing the Turing Test for Drug Discovery, they will act as reliable co-clinicians that automate the heavy lifting of data integration. They will allow human experts to focus on what they do best in auditing findings, guiding strategic direction, and making the final decisions that bring precision, biomarker-driven therapies to the patients who need them most.

.svg)
.svg)


%201%20(1).svg)














.svg)
%20(1).svg)



