Disease Biology
Disease:
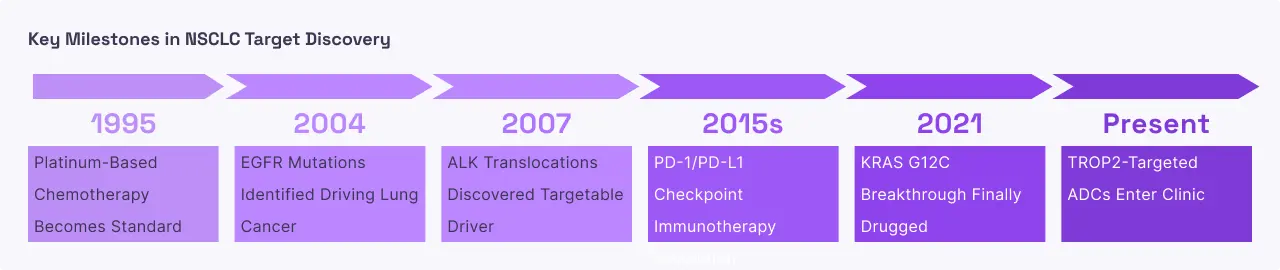
Non-Small Cell Lung Cancer (NSCLC)
Prevalence:
Approximately 2.2 million new lung cancer cases occur globally each year, with non-small cell lung cancer accounting for ~85% of cases.
Disease Mechanism:
Non-small cell lung cancer develops when cells in the lung tissue undergo genetic transformations that allow them to bypass the body's normal growth controls. In a specific subset of these patients, the driving force is a mutation in the EGFR gene itself. These mutations physically change the shape of the receptor's internal engine, making it hyperactive. At a system level, this leads to the formation of tumors that can obstruct the airways and eventually spread through the blood and lymph systems to the brain and bones. Unlike "typical" lung cancers often associated with smoking, EGFR-mutated lung cancer frequently occurs in individuals with little to no smoking history. As the disease progresses, the cancer cells often evolve further, developing new "resistance mutations" that allow them to ignore the very drugs designed to stop them, creating a constant biological arms race between the tumor and the therapy.
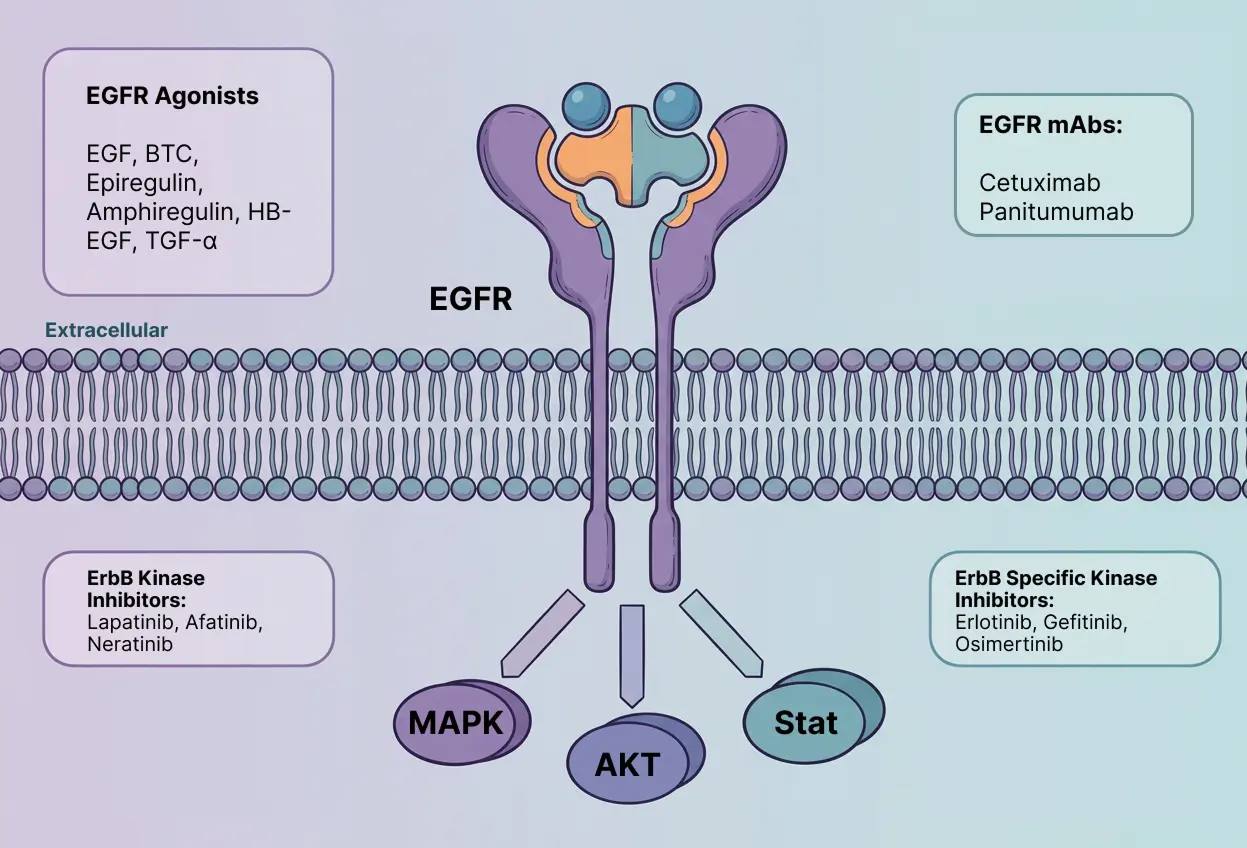
Why target EGFR in Used in NSCLC?
EGFR is the "Achilles' heel" of this specific type of lung cancer. Because the tumor cells are "addicted" to the signals coming from the mutated receptor, shutting it down causes the cells to stop dividing and often triggers them to self-destruct . Targeted therapies called Tyrosine Kinase Inhibitors (TKIs) are designed to fit perfectly into the "fuel pocket" of the mutated receptor, preventing it from processing the energy (ATP) it needs to send signals. This approach is far more precise than traditional chemotherapy; it hits the cancer hard while sparing most healthy cells. Newer generations of these drugs, such as osimertinib, are specifically engineered to overcome common resistance mutations and can even cross the blood-brain barrier to treat cancer that has spread to the brain, significantly extending survival and improving quality of life.
Disease:
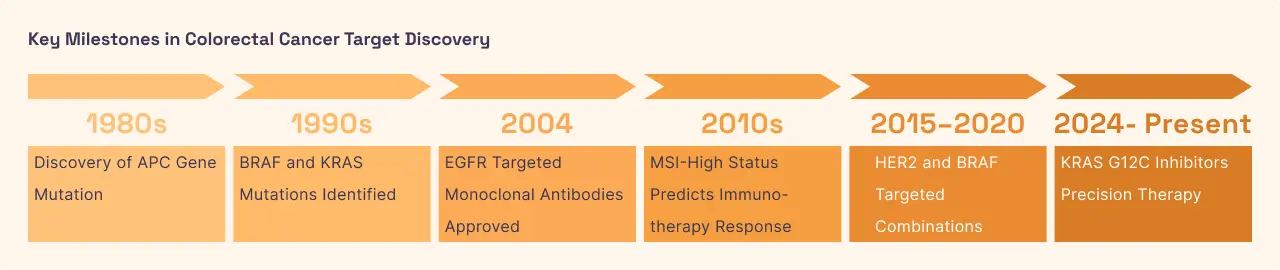
Colorectal Cancer (CRC)
Prevalence:
Approximately 1.9 million new cases each year
Disease Mechanism:
Colorectal cancer arises from the inner lining of the colon or rectum, typically starting as small growths called polyps. While lung cancer is often driven by a mutation in EGFR, colorectal cancer is more frequently driven by an overabundance of normal (wild-type) EGFR proteins on the cell surface. These receptors capture every available growth signal, fueling the tumor's expansion. However, the effectiveness of targeting EGFR in this disease depends heavily on the "wiring" downstream of the receptor. If the proteins further down the signaling chain specifically the RAS and RAF proteins are themselves mutated, they will keep sending growth signals even if the EGFR "antenna" at the top is blocked. This organ-specific cross-talk makes molecular testing of the entire pathway essential for managing the disease as it progresses from local stages to metastatic spread in the liver or lungs.
Why target EGFR in Used in CRC?
In patients whose tumors have a "clean" (wild-type) signaling pathway downstream, blocking EGFR can effectively starve the tumor of the signals it needs to grow. For this disease, doctors typically use monoclonal antibodies, which are large proteins that sit on the outside of the receptor and physically block growth factors from docking. By preventing the receptor from activating, these drugs slow down tumor growth and can even make the tumor more sensitive to traditional chemotherapy. Because this treatment is so specific to the EGFR pathway, it is often used in combination with other drugs to provide a "multi-pronged" attack, particularly for patients with metastatic disease where surgery alone is not enough.



.svg)



.svg)
%201%20(1).svg)
%20(1).svg)
%201%20(1).svg)
.svg)
.svg)



