Disease Biology
Disease:
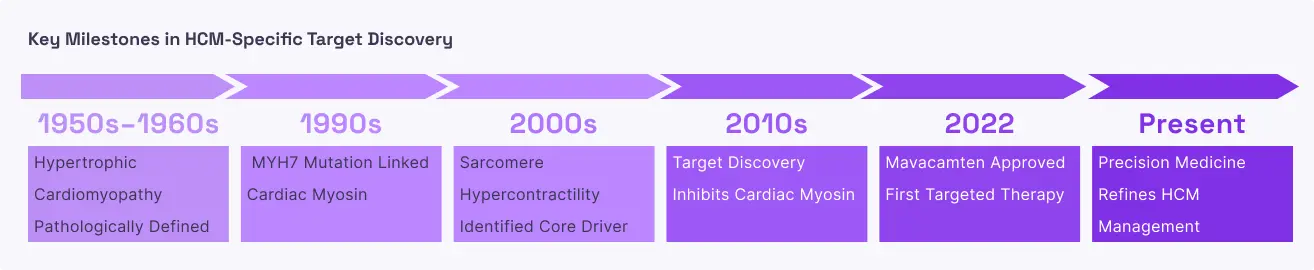
Hypertrophic Cardiomyopathy (HCM)
Prevalence:
~1 in 500 individuals worldwide
Disease Mechanism:
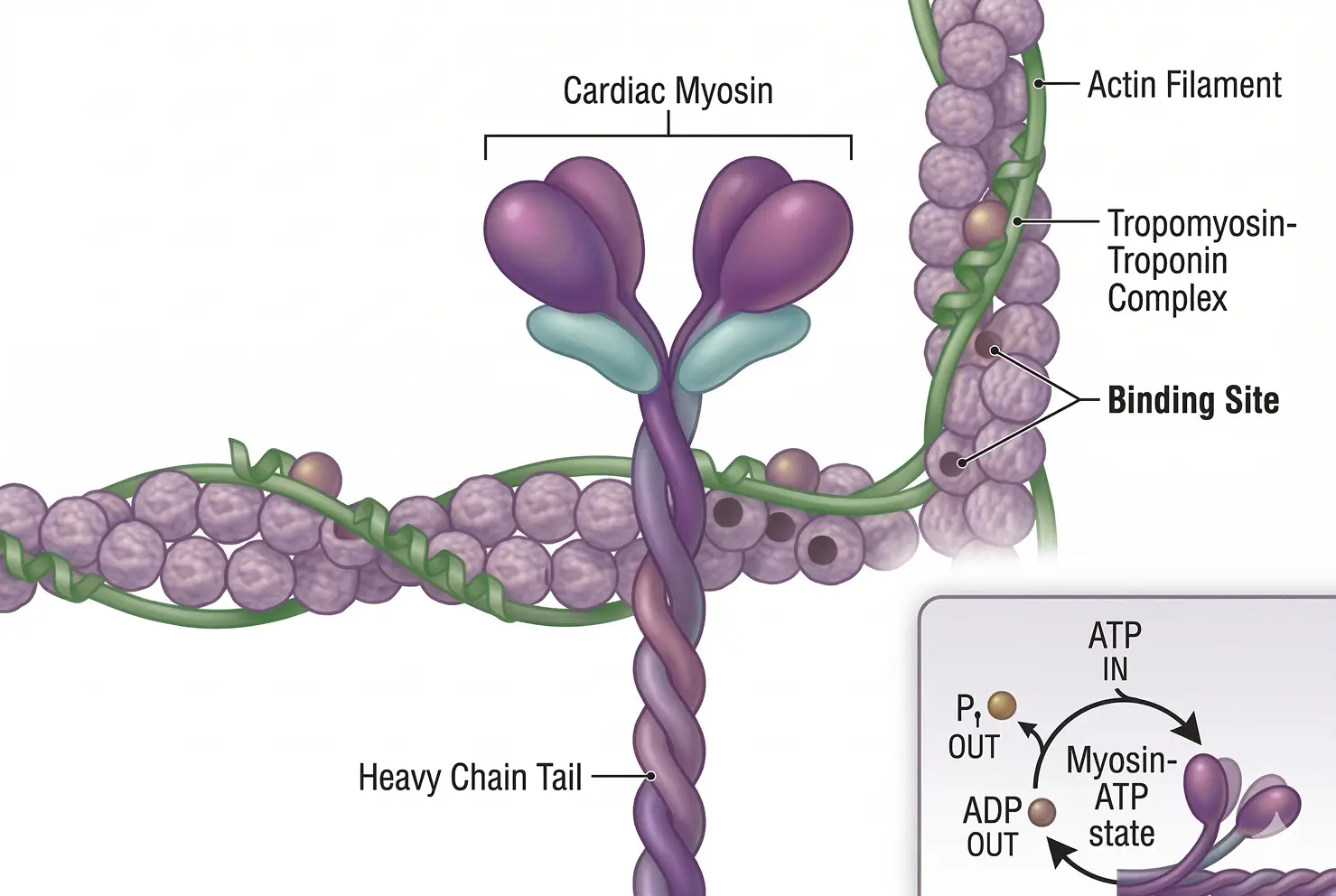
Hypertrophic Cardiomyopathy is a genetic condition where the walls of the heart’s main pumping chamber (the left ventricle) become abnormally thick and stiff. At the molecular level, this is often caused by mutations that leave too many cardiac myosin heads in the "active" state. This leads to a state of chronic over-contraction; the heart muscle is essentially "always on" and working too hard. As the muscle wall thickens, it can physically block the path of blood leaving the heart (known as an obstruction). Over time, this mechanical stress causes the heart tissue to scar (fibrosis), leading to chest pain, shortness of breath, and a high risk of dangerous heart rhythms . The disease is progressive, often beginning with mild symptoms in early adulthood and leading to severe heart failure or sudden cardiac arrest as the heart loses its ability to fill with blood properly.
Why target Cardiac Myosin in HCM?
In HCM, the therapeutic goal is to "calm down" the overactive heart muscle. Cardiac myosin inhibitors work by binding to the myosin motor and shifting it into the "relaxed" standby state. This reduces the number of myosin-actin connections formed during each beat, which effectively thins the overly forceful contraction and allows the heart muscle to relax more completely. Clinically, this relief of tension allows the heart chamber to fill with more blood and reduces the physical obstruction that blocks blood flow to the rest of the body. Unlike older treatments like beta-blockers, which slow down the entire heart rate and can cause fatigue, myosin inhibitors target the specific mechanical defect within the muscle cell itself, improving a patient’s ability to exercise and their overall quality of life.
Disease:
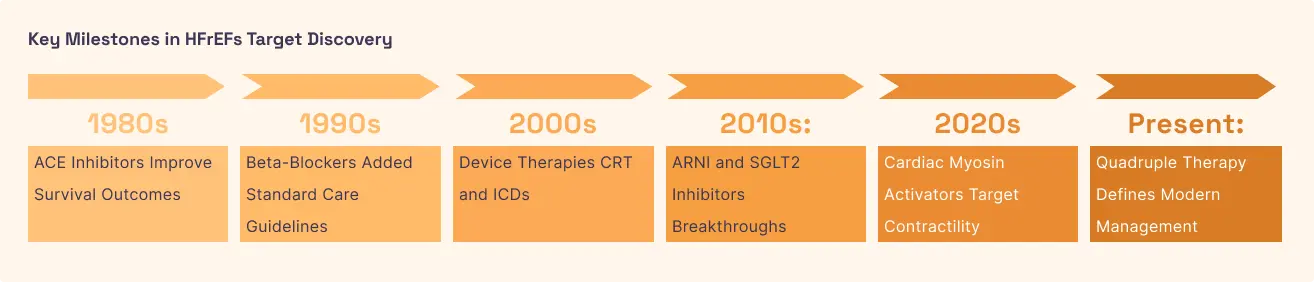
Heart Failure with Reduced Ejection Fraction (HFrEF)
Prevalence:
Approximately 64 million people worldwide
Disease Mechanism:
In Heart Failure with Reduced Ejection Fraction (HFrEF), the heart muscle becomes thin, weak, and dilated. It is the opposite problem of HCM: the heart cannot generate enough force to pump oxygen-rich blood to the body. This weakness is often the result of long-term damage from heart attacks or high blood pressure, which destroys the "motor" units of the heart. The body tries to compensate by pumping faster and releasing adrenaline, but this eventually wears the heart out even further . As the "Ejection Fraction" (the percentage of blood pumped out with each beat) drops, fluid begins to back up into the lungs and limbs, causing the classic symptoms of swelling and extreme breathlessness.
Why target Cardiac Myosin in HFrEF?
For heart failure, scientists use cardiac myosin activators (also called "omecamtiv mecarbil"). Instead of inhibiting the motor, these drugs bind to myosin to increase the duration of time it spends pulling on actin during a contraction. This results in a more productive "stroke" of the heart muscle, increasing the amount of blood pumped out without requiring the heart to use significantly more oxygen or changing the heart's electrical rhythm. This is a major advantage over older "inotropic" drugs, which boosted contraction but often caused fatal arrhythmias by flooding the cells with calcium. By focusing on the myosin motor directly, the therapy aims to strengthen the heart's squeeze in a safer, more sustainable way.



.svg)



.svg)
%201%20(1).svg)
%20(1).svg)
%201%20(1).svg)
.svg)
.svg)



