Disease Biology
Disease:
Small Cell Lung Cancer
Prevalence:
Accounts for approximately 10% to 15% of the 2.3 million global lung cancer cases annually, representing roughly 230,000 to 345,000 new diagnoses [WHO/IASLC].
Disease Mechanism:
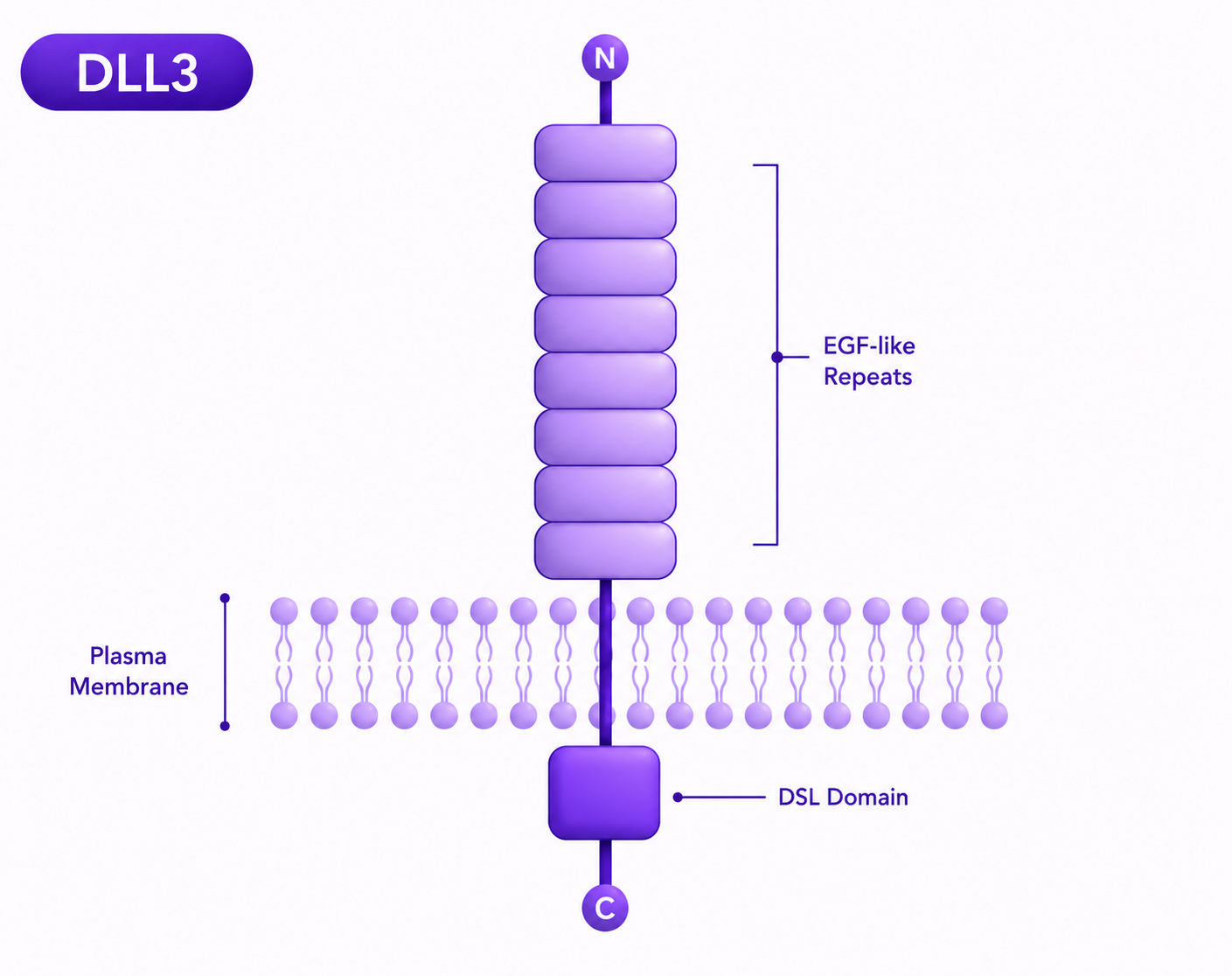
Small cell lung cancer is a highly aggressive tumor characterized by rapid cell doubling, early widespread metastasis, and a distinct neuroendocrine profile. At the systemic level, cells derived from neuroendocrine lineages in the respiratory tract undergo rapid genomic shifts, frequently deleting classic tumor-suppressor pathways. This rapid transformation is accompanied by a dramatic upregulation of surface DLL3. SCLC tumors grow rapidly and easily infiltrate vascular pathways to establish early micro-metastases in the brain, liver, and bones. While highly sensitive to initial platinum-based chemotherapy, SCLC possesses an intrinsic cellular plasticity; the tumor microenvironment quickly adapts, switching cellular phenotypes and altering immune-checkpoint signals to suppress local T-cell responses, leading to rapid disease relapse within months.
Why target DLL3 in Small Cell Lung Cancer
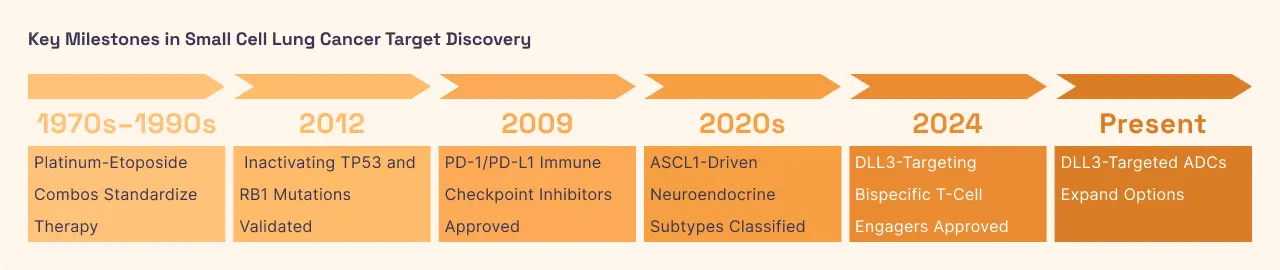
DLL3 is expressed on the surface of roughly 85% of SCLC tumors, making it a near-universal beacon in a disease devoid of other standard driving mutations like EGFR or ALK [9]. Because the local immune environment in SCLC is typically "cold"-meaning it lacks active T-cells to fight the tumor—targeting DLL3 with bispecific T-cell engagers (BiTEs) bridges this gap. These specialized therapies feature one arm that binds tightly to tumor surface DLL3 and another arm that latches onto CD3 on circulating T-cells. This artificial bridge forces an active immune cell directly against the SCLC cell, bypassing the tumor's camouflage systems. This direct mechanical activation triggers targeted tumor lysis and provides a vital therapeutic advantage in patients who have relapsed after standard chemoimmunotherapy.
Disease:
Extrapulmonary Neuroendocrine Carcinomas
Prevalence:
Comprises approximately 2% to 5% of all neuroendocrine neoplasms, with an estimated global incidence of 40,000 cases annually [NORD/AHA]
Disease Mechanism:
Extrapulmonary neuroendocrine carcinomas are rare, poorly differentiated cancers that arise outside the lungs, most frequently originating in the gastrointestinal tract, pancreas, cervix, or prostate. Similar to their lung-based counterparts, epNECs exhibit an aggressive systemic course where normal glandular architecture is replaced by rapidly proliferating neuroendocrine cells. These tumors exhibit altered notch-pathway dynamics, leading to the presentation of high densities of surface DLL3. The molecular dysfunction drives highly invasive growth patterns into surrounding pelvic or abdominal organs. Because of their rarity and biological heterogeneity across different organ sites, systemic management has historically been forced to rely on generalized lung-cancer chemotherapy protocols, which yield short-lived responses and poor definitive outcomes.
Why DLL3 in Extrapulmonary Neuroendocrine Carcinomas
The high expression of DLL3 across various epNECs provides a unifying, tissue-agnostic mechanism to treat these disparate diseases. Rather than tailoring treatments to the organ of origin (e.g., prostate vs. cervix), therapeutics target the common neuroendocrine lineage marked by DLL3. Utilizing newly developed DLL3 antibody-drug conjugates (ADCs) allows for targeted internal delivery of topoisomerase inhibitors or other cellular poisons directly into epNEC cells. Once internal processing releases the chemical payload, it destroys the host cell DNA and can leak across to eliminate adjacent tumor cells via the bystander effect. This mechanism is crucial for overcoming the heterogeneous tumor patches common in advanced abdominal or pelvic metastases.




.svg)



.svg)
%201%20(1).svg)
%20(1).svg)
%201%20(1).svg)
.svg)
.svg)



